1a. Pathophysiological basis and effects of hyper and hypo secretion states of the pit hormones
POSTERIOR PITUITARY: ADH aka Vasopressin
- ADH Excess- SIADH (lots of water is reabsorbed into plasma hence urine vol is low and concn is high)
- concentrated urine = inappropriately high urine osmalality
- diluted plasma = low plasma osmolality (<250 mOsm/ kg)
- leads to water intoxification= headache, vomiting, coma, confusion due to increased intracranial pressure
- leads to hyponatremia
- volume expansion due to increased ECF volume of more than 10%
- decreased aldosterone secretion
- Increased sodium secretion (salt wasting)
- dilutional hyponatremia -> absolute hyponatremia
- Diagnosis of SIADH:
- Inappropriate high urine osm (blood sample very concentrated)
- Low plasma osm
- hyponatremia
- No need to measure serum AVP
- Management
- Restrict water intake
- Block renal action of AVP by administering
- demeclocycline: interferes with cAMP production
- V2 receptor antagonists: acts on CDs
- Replace sodium lost through urine
- treat the cause of SIADH
- Ectopic production of AVP by carcinoma of the lungs, pancreas
- CNS: trauma, infections, tumours
- Drug induced: chlopropamide, nicotine, morphine
- Deficiency- DI (very little water is reabsorbed into plasma hence urine vol is high and concn is low; plasma volume is very low = high osmolality)
- Cranial (Central/ Neurogenic) DI: defective/ decreased production of AVP by the hypothalamus-neuropophyseal system (hypothalamus/ pituitary)
- Nephrogenic DI:
- defective renal response to AVP (hormone resistance)
- defective V2 AVP receptors in the kidneys (receptor disease)
- defective water channel proteins (aquaporins)
SIADH
- retention of water in excess of solutes in the body
DI
- Water diuresis -> polyuria
- Increase plasma osmolality and decrease plasma volume -> Thirst centre in the hypothalamus and leads to thirst and polydipsia
2. Primary, secondary and tertiary dysfunction
Endocrinopathies are classified as primary, secondary, or tertiary.
- Primary endocrine disease inhibits the action of downstream glands/ target endocrine glands.
- Secondary endocrine disease is indicative of a problem with the pituitary gland.
- Tertiary endocrine disease is associated with dysfunction of the hypothalamus and its releasing hormones.
3. Principles underlying the basal and dynamic tests for Hypothalamus-Hypophysis-target endocrine gland axis dysfunction
4. Principles underlying stimulation and suppression tests
Dynamic tests for AVP
- Raise plasma osm and monitor with
- plasma AVP secretion increases
- To increase plasma osm
- water deprivation
- infusion of hypertonic saline
Stimulus for AVP secretion
- increased plasma osm
- decreased plasma volume and decreased BP
Water deprivation test to confirm if it's cranial or nephrogenic DI
- Conducted for 8 hours during the day
- serum and urine osm and body weight recorded every 2 hours up to 8 hours
- fluid is not given during the test
- DI diagnosed if
- serum osm rises to >305mOsm/ kg (normal is from 275-295) AND
- urine osm remains low <300 mOSM/ kg - failure of antidiuresis
- To differentiate between cranial and nephronegic DI
- administer synthetic AVP analogue called DDAVP through IM (des-amino-des-aspartate AVP aka desmopressin) which has more renal effect than vasoconstrictor effect
- If urine now becomes concentrated due to actions of DDAVP on distal nephron -> Cranial DI
- If urine still fails to concentrate as distal nephron is unresponsive to DDAVP -> Nephrogenic DI
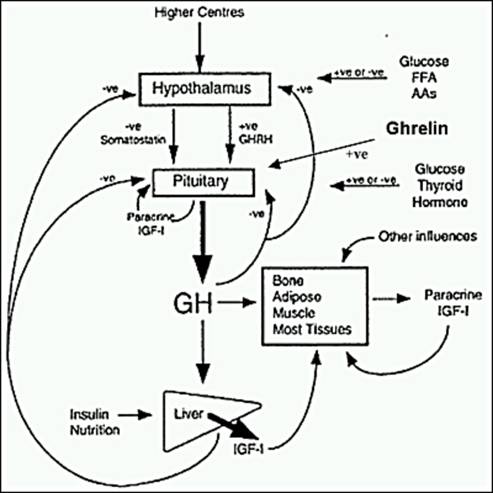
1b. Pathophysiological basis and effects of hyper and hypo secretion states of the pit hormones
ANTERIOR PIT: GH and Prolactin
Dwarfism
- Due to GH deficiency
- Present with systemic illness
- deprivation/ psychosocial dwarfism: mental retardation
- late/ no pubertal development
- low IQ
- unproportionate body
- Laron dwarfs
- hGH receptor defect in liver leading to decreased IGF-1 release leading to decreased growths
- GH levels are normal
- But they are not as short as pituitary dwarfs
- Lab tests
- measure serum GH levels after stimulating the growth hormone secretion -> dynamic provocative (stimulation) tests
- Insulin tolerance test (gold standard)- induce hypoglycaemia (metabolic stress) - under normal response, blood glucose will fall and stimulates secretion of serum GH; also when blood glucose falls, it stimulates increase in serum ACTH and cortisol levels HENCE ITT is also used to evaluate hypothalamus-hypophyseal-adrenocortical axis
- Post exercise blood sample - induce physical and mental stress -> release GH
- GHRH stimulation test
- Test for GH levels after 1 hour going to sleep
- Glucagon - less reliable than ITT
- Arginine
- Clonidine
- If serum levels of GH increased -> enough reserve
- If not -> not enough reserve -> deficiency of GH
Gigantism (child)/ Acromegaly (adult)
- ** patient with GH secreting adenoma that started before puberty and presents after epiphyseal closure will have features of gigantism and acromegaly
- Due to hypersecretion of GH
- Signs and symptoms
- Lab tests
- Raised serum GH and IGF-1
- Absence of nocturnal rise of GH (GH levels raised all the time)
- Suppression test: Oral Glucose Tolerance Test
- Normal: hyperglycaemia will suppress GH
- Failure to suppress GH levels -> acromegaly
- Neuroradiological assessment of the effect of pit tumour
Hyperprolactinaemia
- Functions of prolactin
- Promotes lactation
- prolactin causes breast development during pregnancy, together with other hormones eg oestrogen
- prolactin causes milk formation and secretion from the breast (prolactin increase action of mRNA -> promotes synthesis of milk proteins eg casein and lactalbumin)
- Antigonadotrophic effect
- inihibits effects of gonadotropins, leading to
- lactational amenorrhea
- birth spacing
- in males: impotence
- Clinical signs and symptoms
- galactorrhea
- hypogonadism -> amenorrhea, infertility
- Lab tests
- basal plasma prolactin levels are raised (but must exclude stress, pregnancy and drugs)
- dynamic tests are not useful in Ddx
- Neuroradiological assessment of the effect of pit tumour
5. Evaluation of Hypothalamus-Hypophysis-target endocrine gland axis activity (clinical, lab-hormone assays, imaging, special investigations
Hormones regulate their plasma concentration through negative feedback along the axis
- short loop (hormones released by ant. pituitary, eg TSH inhibits hypothalamus to release TRH)
- long loop (hormones released by target endocrine glands eg T4 or T3, inhibits ant pituitary and hypothalamus to secrete TRH and TSH
Hypothyroidism
Primary defect: T3 & T4 low, TSH and TRH normal
Secondary defect: T3 & T4 low, TSH low and TRH normal
Tertiary defect: all low
Eg defective thyroid gland - decreased T4, increased TSH and TRH
To check if it's hypothalamic or pituitary defect, use TRH stimulation test by giving injections of TRH and measure serum TSH
- If serum TSH increases - pituitary is normal -> hypothalamic defect
- If serum TSH doesn't increase -> pituitary defect
Congenital Hypothyroidism -> Cretinism
- normally due to maternal iodine deficiency
- Large tongue
- Coarse features
- Mental retardation
- Large anterior fontanelle
- Small stature
- Decreased activity
- Umbilical hernia
- Mottled, cool, dry skin
Treatment
Administer serum TSH
- if thyroid gland is normal -> will secrete T4
- but if thyroid gland is not -> less T4 or no T4 is secreted
- Require Thyroid Hormone replacement therapy
Hyperthyroidism
Primary hyperthyroidism : increased T4 and T3 but decreased TSH and TRH
Secondary/ Tertiary hyperthyroidism: increased T4 and T3, increased TSH but decreased TRH
Secondary/ Tertiary hyperthyroidism: All increased
T3 suppression test
- Large dose of T3 administered
- Normal: Negative feedback to pituitary and hypothalamus to reduce secretion of TRH and TSH
- If fails to suppress TSH secretion -> functional tumours
Panhypopituitarism
The sequence of loss of hormonal secretion:
1. hGH
2. LH (secondary hypogonadism)
3. FSH
4. ACTH (secondary adrenal insufficiency)
5. TSH (secondary hypothyroidism)
Causes
1. Genetics
2. Nine Is (Infarction (Sheehan's syndrome), Invasive, Infiltrative, Injury, Immunologic, Iatrogenic, Infectious, Idiopathic and Isolated)
Investigations
- Stimulations tests for
- hGH (GHRH test, ITT)
- LH, FSH (GnRH test)
- ACTH (CRH test, ITT)
- TSH (free T3, T4/ TSH/ TRH)
- Or the combination of the above: sequential injections of GHRH, CRH, GnRH and then measure serum GH< ACTH, LH and FSH